Vaccine
Talk
(Egyptian Edition)
"Everything you need to know about
vaccines in Egypt"
(Egyptian Edition)
"Everything you need to know about
vaccines in Egypt"
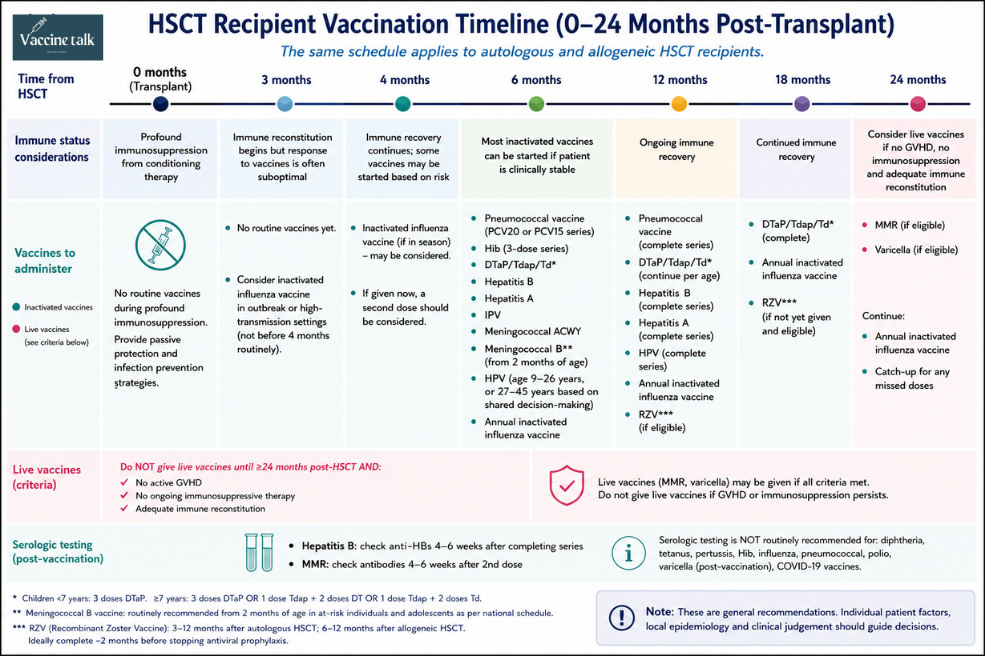
Revaccination guidance for autologous and allogeneic HSCT recipients — inactivated schedules, live vaccine timing, serology, and travel vaccines.
Recipients of haematopoietic stem cell transplants (HSCT) are at increased risk of vaccine-preventable diseases due to prolonged immunosuppression and the loss of pre-existing immunity. Both autologous and allogeneic HSCT recipients may lose protective immunity acquired through previous vaccination or natural infection, making revaccination an essential component of post-transplant care.
HSCT involves the administration of hematopoietic-ablative therapy followed by the infusion of stem cells obtained either from the recipient (autologous transplant) or from a donor (allogeneic transplant). Stem cells may be collected from:
Although autologous HSCT recipients generally recover immune function more rapidly than allogeneic recipients, both groups require systematic revaccination after transplantation.
Immunosuppression following HSCT results from several factors:
As immune reconstitution occurs, immunologic memory from previous vaccinations gradually declines. Antibody levels against vaccine-preventable diseases such as tetanus, poliovirus, measles, mumps, rubella, and infections caused by encapsulated bacteria may decrease significantly within 1–4 years after transplantation if revaccination is not performed.
Chronic GVHD is associated with persistent immune dysfunction and functional hyposplenism, resulting in increased susceptibility to infections caused by encapsulated organisms, particularly Streptococcus pneumoniae.
Patients with chronic GVHD who remain on immunosuppressive therapy may also require antibiotic prophylaxis in addition to vaccination.
Because immune recovery varies substantially between individuals, recommendations regarding live vaccines depend on the patient's degree of immune reconstitution and immunosuppressive status.
Current guidelines generally recommend the same revaccination schedule for both autologous and allogeneic HSCT recipients regardless of:
Even patients who completed routine vaccinations before transplantation should be considered for revaccination because protective immunity may be lost after HSCT.
Most inactivated vaccines are restarted approximately 6 months after transplantation, although certain vaccines may be initiated earlier in selected circumstances.
HSCT recipients are at particularly high risk for invasive pneumococcal disease.
Revaccination is recommended regardless of prior pneumococcal vaccination history.
Preferred Schedule
PCV20
Start 3–6 months after HSCTFour-dose series
Alternative Schedule
PCV15
Three doses given 4 weeks apart
Followed by PPSV23
GVHD note
For patients with GVHD, a fourth dose of PCV15 is recommended instead of PPSV23.
Children <7 Years
DTaP
Three-dose DTaP series
Individuals ≥7 Years
DTaP / Tdap / Td
Acceptable schedules include:
Preferred schedule
For previously unvaccinated patients older than 6 years, a schedule consisting of one dose of Tdap followed by two doses of Td is generally preferred.
Revaccination against hepatitis B is recommended after HSCT. Because vaccine response may be impaired, post-vaccination serologic testing should be performed approximately 4–6 weeks after completion of the vaccine series to assess protection and determine whether additional doses are needed.
Hepatitis A vaccine should be re-administered according to post-transplant vaccination recommendations and may be particularly important for individuals at increased risk or those planning international travel.
Revaccination with IPV is recommended because immunity to poliovirus may decline following transplantation.
Revaccination is recommended for:
Vaccine types
MenACWY & MenB
This includes both:
HPV vaccination should be administered according to age-based recommendations:
RZV may be administered after immune recovery:
Ideally, vaccination should be completed approximately 2 months before discontinuation of antiviral prophylaxis when such therapy is being used.
Live vaccines should not be administered routinely during the first 24 months after HSCT.
Live vaccines may be considered only if all of the following conditions are met:
MMR vaccine may be administered under the above conditions. Serologic testing is recommended approximately 4–6 weeks after the second dose because antibody levels may guide the need for additional vaccination.
Varicella vaccine may be considered when the same eligibility criteria for live vaccines are met. Post-vaccination varicella serology is not recommended because currently available commercial assays are insufficiently sensitive to detect vaccine-induced immunity.
The following live vaccines are generally contraindicated after HSCT:
These vaccines should not be administered to HSCT recipients.
Some vaccines are not routinely indicated but may be required depending on travel plans, occupational exposure, or individual risk factors.
These include:
Yellow fever revaccination
For individuals who received yellow fever vaccine before HSCT, revaccination may be required after transplantation when travel-related risk exists and immune competence has been restored.
Specialist consultation
Specialist consultation is recommended before administering any travel-related vaccine to HSCT recipients.
Assessment of vaccine response is recommended:
Clinical use of results
Results may guide the need for additional vaccine doses.
Routine serological testing is not recommended for:
Vaccination of stem cell donors before stem cell collection has been shown to improve early antibody responses in recipients for certain vaccines, including:
However, practical, logistical, and ethical considerations often limit routine implementation of donor immunization strategies.